Table Of Content
- What are quasi-experimental research designs?
- Get help with access
- Workplace financial education and change in financial knowledge: A quasi-experimental approach (Horwitz et al.,
- What Are the Different Quasi-experimental Study Designs?
- Knowledge and skills for financial decision making-Low-Favorable impacts
- Quasi-experimental Designs That Use Control Groups and Pretests
In the four-year period of IJMI publications reviewed by the authors, nine quasi-experimental studies among eight manuscripts were published. Of these nine, five studies were of category A, one of category B, one of category C, and two of category D. Two of the nine studies (22%) mentioned at least one of the potential limitations of the quasi-experimental study design. For medical informatics interventions, it is often difficult to randomize the intervention to individual patients or to individual informatics users. So while this randomization is technically possible, it is underused and thus compromises the eventual strength of concluding that an informatics intervention resulted in an outcome. For example, randomly allowing only half of medical residents to use pharmacy order-entry software at a tertiary care hospital is a scenario that hospital administrators and informatics users may not agree to for numerous reasons.
What are quasi-experimental research designs?
(PDF) A quasi-experimental study to assess the effectiveness of structured teaching programme regarding BE FAST ... - ResearchGate
(PDF) A quasi-experimental study to assess the effectiveness of structured teaching programme regarding BE FAST ....
Posted: Mon, 04 Mar 2024 08:00:00 GMT [source]
The study used a non-randomized selection process to determine which city would participate in the research. Researchers left out certain variables that would play a crucial role in determining the growth of each city. They used pre-existing groups of people based on research conducted in each city, rather than random groups. Recruiting participants and properly designing a data-collection attribute to make the research a true experiment requires a lot of time and effort, and can be expensive if you don’t have a large funding stream.
Get help with access
In this article we review the use of experimental designs in implementation science, including recent methodological advances for implementation studies. We also review the use of quasi-experimental designs in implementation science, and discuss the strengths and weaknesses of these approaches. This article is therefore meant to be a practical guide for researchers who are interested in selecting the most appropriate study design to answer relevant implementation science questions, and thereby increase the rate at which effective clinical practices are adopted, spread, and sustained. QEDs test causal hypotheses but, in lieu of fully randomized assignment of the intervention, seek to define a comparison group or time period that reflects the counter-factual (i.e., outcomes if the intervention had not been implemented) (43).
Workplace financial education and change in financial knowledge: A quasi-experimental approach (Horwitz et al.,
Individuals contributed follow-up time to the “pre-clinic” phase from the baseline date established for the cohort until the actual date of their first clinic visit, and also to the “post- clinic” phase thereafter. "Quasi-experimental research is similar to experimental research in that there is manipulation of an independent variable. It differs from experimental research because either there is no control group, no random selection, no random assignment, and/or no active manipulation." Another problem with quasi-experiments is the natural progression of the disease or the condition under study — When studying the effect of an intervention over time, one should consider natural changes because these can be mistaken with changes in outcome that are caused by the intervention.
What Are the Different Quasi-experimental Study Designs?
Of these 25, 15 studies were of category A, five studies were of category B, two studies were of category C, and no studies were of category D. Although there were no studies of category D (interrupted time-series analyses), three of the studies classified as category A had data collected that could have been analyzed as an interrupted time-series analysis. Nine of the 25 studies (36%) mentioned at least one of the potential limitations of the quasi-experimental study design.
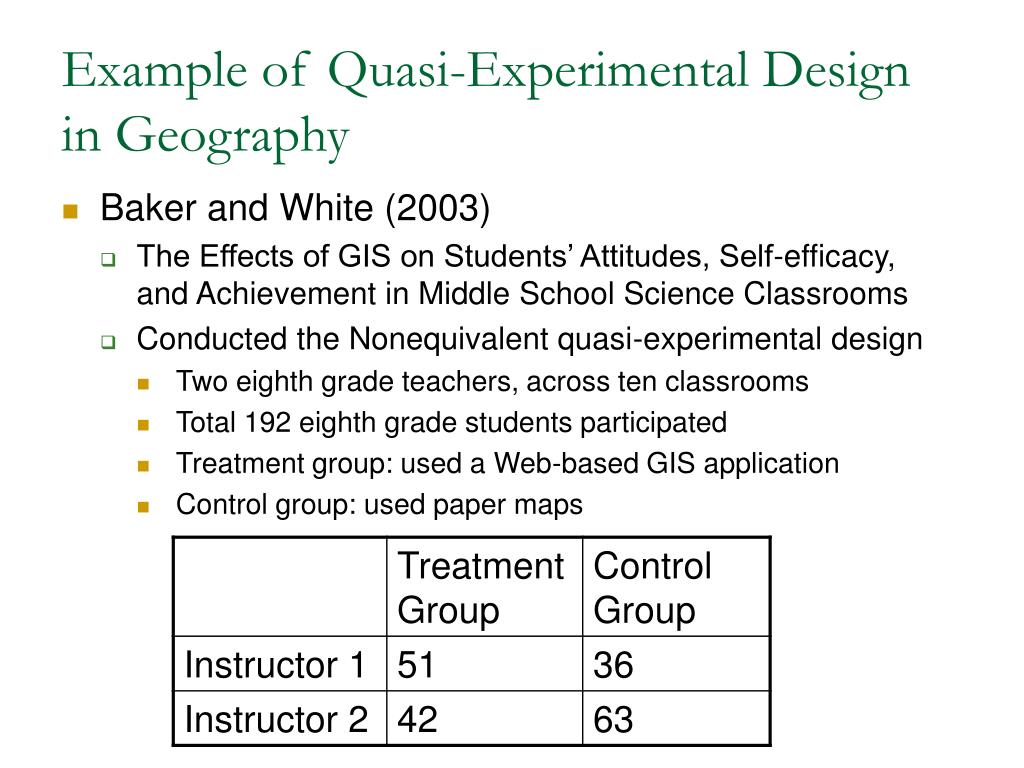
The comparison group consisted of non-participants identified by employers and received a financial education booklet in lieu of classes. The comparison group consisted of 56 employees, 7 from Company A and 49 from Company B. The study sample was predominantly female, and a plurality of employees had incomes between $38,521 and $101,582. However, the comparison group members had a lower percentage of bachelor’s degree recipients than the program group. A type of quasi-experimental design that is generally better than either the nonequivalent groups design or the pretest-posttest design is one that combines elements of both. There is a treatment group that is given a pretest, receives a treatment, and then is given a posttest.
But at the same time there is a control group that is given a pretest, does not receive the treatment, and then is given a posttest. The question, then, is not simply whether participants who receive the treatment improve but whether they improve more than participants who do not receive the treatment. The advantage of this design is that it demonstrates reproducibility of the association between the intervention and the outcome. For example, the association is more likely to be causal if one demonstrates that a pharmacy order-entry system results in decreased pharmacy costs when it is first introduced and again when it is reintroduced following an interruption of the intervention.
Quasi-experimental Designs That Use Control Groups and Pretests
Thus, if the average length of stay did not change following the intervention but pharmacy costs did, then the data are more convincing than if just pharmacy costs were measured. Because they allow better control for confounding variables than other forms of studies, they have higher external validity than most genuine experiments and higher internal validity (less than true experiments) than other non-experimental research. SMARTs are multistage randomized trials in which some or all participants are randomized more than once, often based on ongoing information (e.g., treatment response). In implementation research, SMARTs can inform optimal sequences of implementation strategies to maximize downstream clinical outcomes.
Example 2: Determining the effectiveness of teaching modern leadership techniques in start-up businesses
Participants on either side of the cutoff point are then compared to determine whether the intervention or event had an effect. Having a control group is not required, but if present, it provides a higher level of evidence for the relationship between the intervention and the outcome. All original scientific manuscripts published between January 2000 and December 2003 in the Journal of the American Medical Informatics Association (JAMIA) and the International Journal of Medical Informatics (IJMI) were reviewed. Other authors (ADH, JCM, JF) then independently reviewed all the studies identified as quasi-experimental.
When this is the case, additional designs for the intervention roll-out, such as adaptive or hybrid designs can also be considered. In this design, all subjects receive the new PDA-based order entry system and the old computer terminal-based order entry system. The counterbalanced design is a within-participants design, where the order of the intervention is varied (e.g., one group is given software A followed by software B and another group is given software B followed by software A). The counterbalanced design is typically used when the available sample size is small, thus preventing the use of randomization. This design also allows investigators to study the potential effect of ordering of the informatics intervention. These designs are frequently used when it is not logistically feasible or ethical to conduct a randomized controlled trial.

Human service professionals planning to undertake a program evaluation of their own agency's services will find this book of immense help in understanding the steps and actions needed to adopt a quasi-experimental strategy. It is usually the case that ethical and pragmatic considerations preclude the use of randomly assigning social work clients to experimental and comparative treatment conditions, and in such instances, the practicality of employing a quasi-experimental method becomes an excellent alternative. We then performed a systematic review of four years of publications from two informatics journals.
For example, Kirchner and colleagues (2014) used this type of design to evaluate the integration of mental health services into primary care clinics at seven US Department of Veterans Affairs (VA) medical centers and seven matched controls. As well, when a complex intervention is related to a policy or guideline shift and implementation requires logistical adjustments (such as phased roll-outs to embed the intervention or to train staff), QEDs more truly mimic real world constraints. As a result, capturing processes of implementation are critical as they can describe important variation in uptake, informing interpretation of the findings for external validity. However, QEDs are often conducted by teams with strong interests in adapting the intervention or ‘learning by doing’, which can limit interpretation of findings if not planned into the design. As done in the study by Bailet et al (3), the investigators refined intervention, based on year 1 data, and then applied in years 2–3, at this later time collecting additional data on training and measurement fidelity. This phasing aspect of implementation generates a tension between protocolizing interventions and adapting them as they go along.








No comments:
Post a Comment